June 19, 2015
Looking Inside the Biotech Black Box (Part 11)
Cost-Effectiveness and Affordability of New Medicines (4)
Can individuals, healthcare payers and society in general afford to pay for all of the new diagnostics, drugs and medical procedures?

In the last blog, I concluded that the use of the new Hepatitis C drugs was cost-effective in the patient groups in which it had been tested. In a previous blog, I stated that physicians wanted to provide their choice of the best available care regardless of the cost – which means that they may want to treat all patients with Hepatitis C infections with the new drugs. Gilead Sciences has a quote from the AASLD (American Association for the Study of Liver Diseases) on their Q1 2015 slide deck:
“Evidence clearly supports treatment of all HCV-infected persons except those with limited life expectancies ….”
Gilead treated 91,000 persons in Q1 – cumulative to end of Q1 was 260,000 persons. This slide deck also states that there are 6.6 M infected persons in the major developed countries – 4.0 M of which are in the U.S. If all these people were treated for 84 days at US$1,000 per day, the total cost would be US$554.4 billion – the global pharmaceutical market is only about US$1,000 billion annually. This huge number moves the discussion from cost-effectiveness to affordability.
Of every 100 people infected with the Hepatitis C virus, about
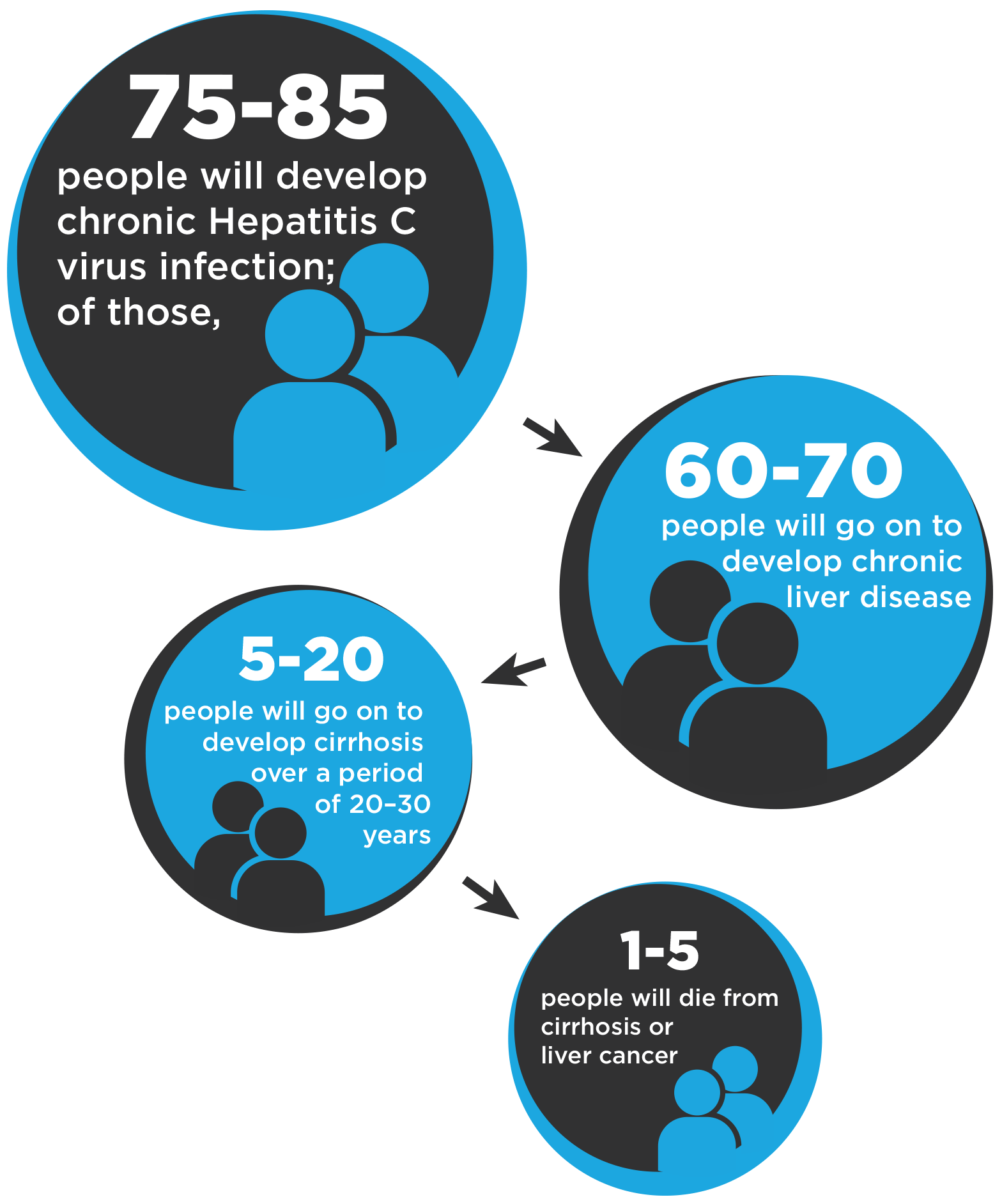
This information is from the U.S. CDC and it triggers many questions.
Some infected persons clear the acute infection and never develop a chronic Hepatitis C infection.
- Can they be identified reasonably soon after infection?
- Do they require any medical care as a result of the acute infection?
- Do they require frequent diagnostic monitoring as a result of the acute infection?
The remainder of the infected persons will develop a chronic Hepatitis C infection.
- What is the impact on quality-of-life for a person with a chronic infection?
- Can this group of patients be stratified in any way soon after infection?
- Can this group be diagnostically monitored at a reasonable cost to determine the rate and extent of progression to chronic liver disease, including cirrhosis and liver cancer?
While the proper ethical and moral decision might be to treat all chronic Hepatitis C patients after diagnosis, it is a financial impossibility for the healthcare systems.
Therefore, treatment criteria will be imposed on physicians by the healthcare system under which they are reimbursed.
- Should all patients be first treated with an interferon-based drug regimen?
- Should all patients who fail to achieve an SVR on an interferon-based drug regimen be automatically transferred to one of the new drug regimens?
- Should all patients be treated with one of the new drug regimens when cirrhosis or other liver damage is first diagnosed?
- Should patients with liver cancer be treated since the cure rate for liver cancer is so low?
The treatment of the vast majority of Hepatitis C patients will be paid for through taxes (less so in the U.S.). Taxes are imposed by politicians who, from my cynical perspective, are mostly interested in getting re-elected in a few years. Politicians do not like raising taxes at more than the rate of inflation except for things which will benefit most of their voters.
- Are the 99% of voters who are not infected willing to pay for the 1% who are infected?
- If a proposal is made to treat an incremental group of infected people, will this require increased taxes, cuts elsewhere in the healthcare system or cuts in other public services?
For patients covered by non-government insurance plans, some of the insurance companies just manage the claims process. For other insurance companies, healthcare insurance is treated in the same way as auto and property insurance. There are numerous press reports of cases where access to the new drugs is denied as ‘not medically necessary’. In one case, a woman wanted to be cured of hepatitis C so she could have a baby with no chance of passing on the virus to her baby.
There are no easy answers!!

Alzheimer’s disease (AD) is the most common form of dementia, is progressive and symptoms include memory loss, confusion, and behavior changes. The currently approved drugs do not alter the course of the disease but simply increase the activity in the parts of the brain which are still working. Virtually every adult in the developed world has a family member or family friend who has or will experience the devastation caused by this disease.
Aducanumab (BIIB037) is being developed by Biogen for the treatment of AD. BIIB037 is a human recombinant monoclonal antibody selected from a population of elderly, healthy donors and cognitively stable patients, which targets aggregated forms of beta amyloid deposited into the amyloid plaque in the brain of AD patients. The drug is administered through monthly iv infusions. Biogen recently stated that it will be moving its Alzheimer’s drug BIIB037 into Phase 3 clinical trials based on an interim look in a Phase 1 trial which showed both a reduction in beta amyloid in the brain and improved cognition in patients with early signs of the disease 54 weeks after starting treatment.
While there is a graveyard full of the clinical failures in AD, the disease is so devastating for the patients and families that almost any clinical improvement is likely to be approved. A key question is whether the healthcare system can afford to pay for a drug which has a small clinical impact.
The range of clinical outcomes for this drug and other AD treatments might include:
- A statistically significant positive outcome only in patients with a specific metabolic or genetic profile;
- Modest increase in cognition which is maintained for a few months to 2 to 3 years before the disease starts to progress again;
- No change in cognition for a few years before the disease starts to progress; and
- A lower rate of decline in cognition for several years.
Assuming that there is a positive clinical outcome and that the annual cost of the drug is $100,000 (pricing is strictly my guess), what are the potential impacts on the healthcare system?
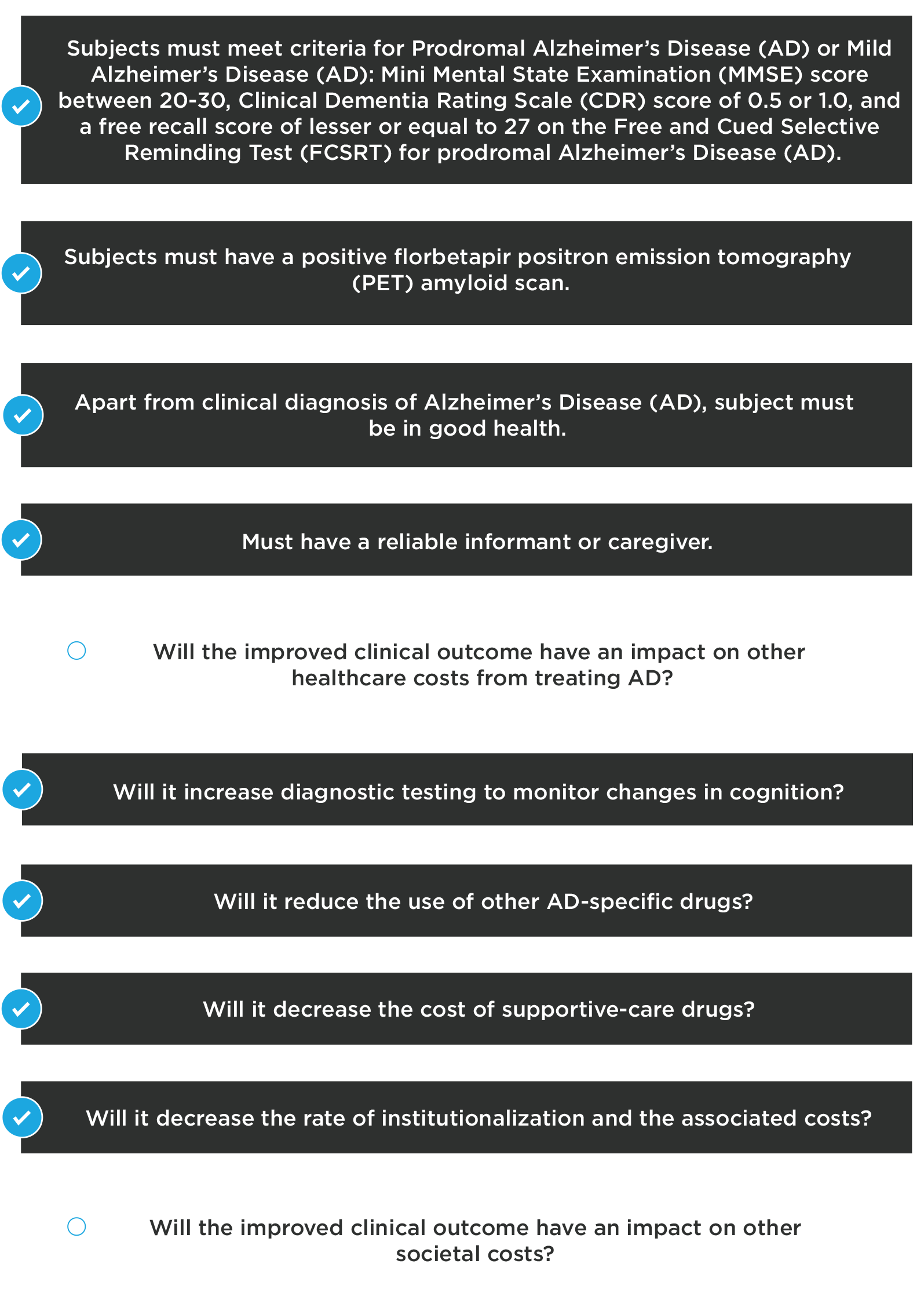
- People will want to be tested earlier if there is a treatment which can impact disease progression. Drug plans will likely try to restrict use to people most likely to benefit in order to control their costs. It is possible that the restrictions may be similar to the inclusion criteria for the Phase 1 study
(see https://clinicaltrials.gov/ct2/show/NCT01677572?term=BIIB037&rank=2).
Key Inclusion Criteria:
There is insufficient information at this time to determine whether this drug is either cost-effective or affordable. However, these are the types of questions which must be asked at the early stages of clinical development for every new drug candidate.
Biotech companies are part of the pharmaceutical industry, which has undergone and will continue to undergo major structural changes. In the next few blogs, we will look at some of these structural changes.
[The author and his immediate family members may have long or short positions in the shares of some companies mentioned in or assessed during the preparation of this blog. Past share price performance may not be an indicator of future share price performance. This blog does not consider the investment objectives, financial situation or particular needs of any particular person. Investors should obtain professional advice based on their own individual circumstances before making an investment decision.]
As with all our posts, please see our full legal disclaimer.


