May 8, 2015
Looking Inside the Biotech Black Box (Part 8)
Cost-Effectiveness and Affordability of New Medicines (1)
There were 5,408 medicines in clinical development globally in December 2011, many of which were being developed for multiple indications (PhRMA, the Pharmaceutical Research and Manufacturers of America; http://www.phrma.org/pipeline). It is possible that up to 1,000 of these medicines will eventually be approved – based on approval rates of 50% for those in Phase 3, 20% for Phase 2 and 10% for Phase 1 (my estimates).
Can individuals, healthcare payers and society in general afford to pay for all of the new diagnostics, drugs and medical procedures? 
New medicines are priced ‘as high as the market will bear’ – this is the universal pricing model for all industries and the pharmaceutical industry should not be any different. However, in most retail and industrial markets, the markets will ask questions and push back on price increases, including assessing the purchase of alternative items. Until about 15 years ago, there was very little resistance from the payers on new drug prices. Two of the countries which refused to blindly accept new drug prices and established review processes were Germany and the U.K. In Germany, insurers follow the assessments of new drugs by the Institute for Quality and Efficiency in Health Care (IQWiG). Like Britain’s National Institute for Health and Clinical Excellence (NICE), Germany’s IQWiG looks at the benefit of using a new drug versus the current standard(s) of care.
There are four questions which need to be addressed.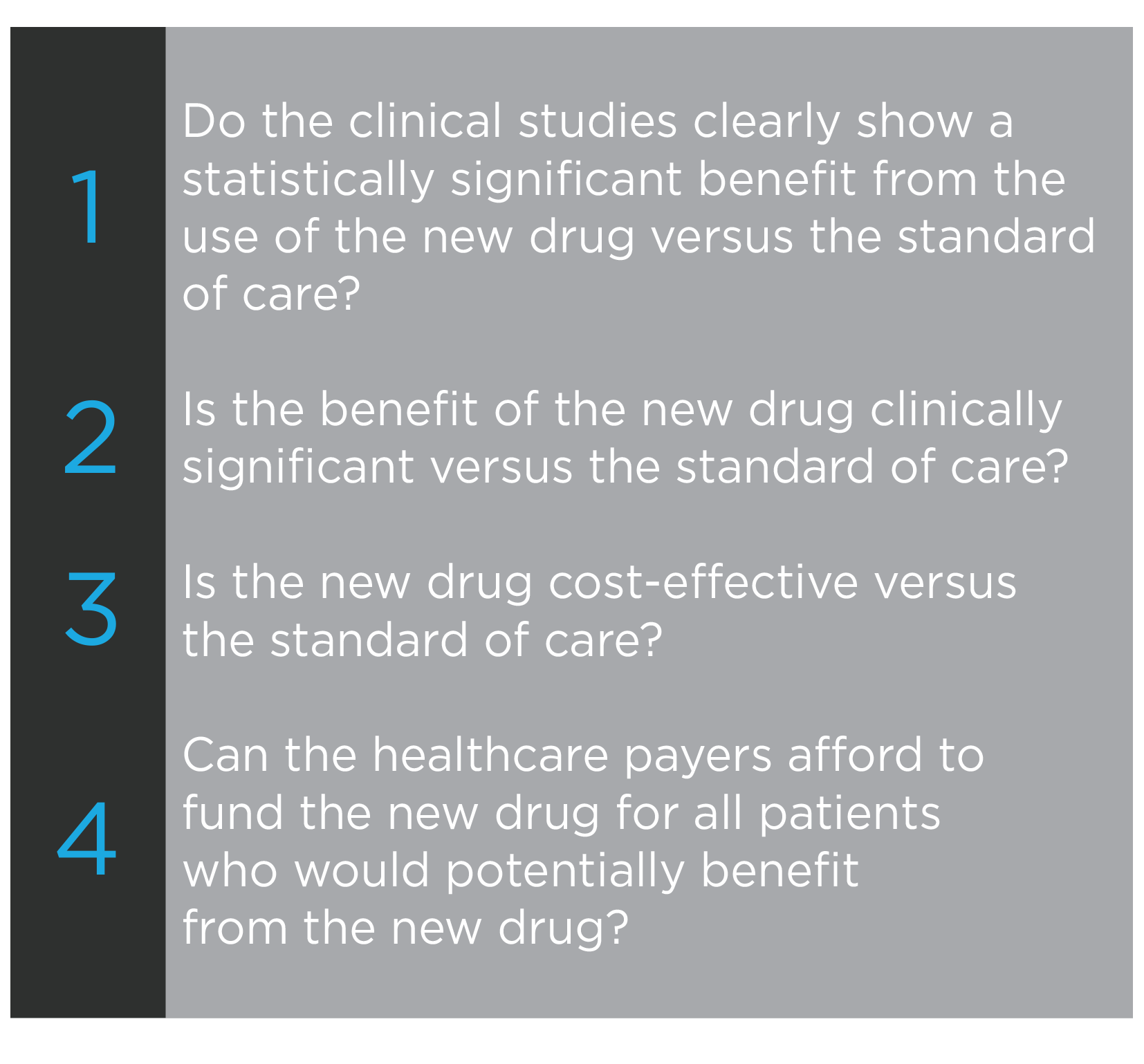
 The first determination of effectiveness is by the drug approval agencies – does the drug have a statistically significant benefit over the standard of care used in the controlled Phase 3 clinical trials. Three major variables in designing Phase 3 clinical trials must be assessed.
The first determination of effectiveness is by the drug approval agencies – does the drug have a statistically significant benefit over the standard of care used in the controlled Phase 3 clinical trials. Three major variables in designing Phase 3 clinical trials must be assessed.
- In many diseases, the endpoint or benefit being assessed is well established. For cancer, the endpoint is either median overall survival (OS) or progression-free survival (PFS). One might think that these two endpoints would be linked with an increase in PFS leading to an increase in OS but this is not true in many cancers and with many drugs. In diseases such as Alzheimer’s, multiple tests are used and the tests are evolving. There are many diseases where there are no approved drugs which means negotiations between the sponsor and the FDA on an acceptable endpoint.
- Determining which patient population will be assessed in clinical trials has changed in the past decade. The old mantra was treat everybody in order to have the largest potential market for the drug. However, testing targeted therapies in a large and heterogeneous patient population may result in a clinical trial failure whereas a trial in a smaller, homogeneous and pre-selected patient population might be successful. However, for a company to have the same financial return in a smaller patient population, the treatment cost per patient may be substantially higher.
- The real standard of care is not determined by the FDA but rather by the physicians who treat the patients, with assistance from their professional associations. A drug could be used clinically with a different dosing or regimen, or even to treat a different disease or stage of disease than was approved by the FDA. This creates a problem for the FDA and companies designing new clinical trials – how can the FDA approve the structure of a clinical trial where the standard of care does not conform to the drug label and physicians will not enroll patients in a trial where they would get less than the standard of care.
Physicians, not the FDA, determine whether a new drug has a clinically significant benefit when used as an alternative to or in combination with the standard of care. They make this determination based on their clinical experience and the clinical data on the new drug. The conclusions they reach are expressed through their prescribing patterns.
Physicians decide on the treatment for each of their unique patients but they get help from groups which create clinical guidelines and run real-life clinical trials, such as the following two cancer-focused organizations.
- The National Comprehensive Cancer Network (http://www.nccn.org/) has clinical practice guidelines for most types of cancer, which includes diagnostic and therapeutic decision-trees.
- The National Cancer Institute (NCI; http://www.cancer.gov/), one of the institutes in the U.S. National Institutes of Health (NIH), has a National Clinical Trials Network which conducts clinical trials both before and after approval of a drug.
The FDA does not govern the prescribing practices of physicians. Physicians are governed by their professional regulatory bodies, at the provincial level in Canada and the state level in the U.S.. Physicians want to keep the ability to treat a patient using the diagnostic tests and drugs which they believe will give the best clinical outcome regardless of the cost. Those last four words were not a problem before the arrival of the first blockbuster drugs in the 1980s. There was some concern when the cancer drug paclitaxel was approved in 1992 with an annual treatment cost of about US$10,000. There is now a major concern when virtually every new cancer drug carries an annual price tag of about US$100,000.
In the next blog, we will assess the last two questions and look at the cost-effectiveness and affordability of new medicines.
[The author and his immediate family members may have long or short positions in the shares of some companies mentioned in or assessed during the preparation of this blog. Past share price performance may not be an indicator of future share price performance. This blog does not consider the investment objectives, financial situation or particular needs of any particular person. Investors should obtain professional advice based on their own individual circumstances before making an investment decision.]
As with all our posts, please see our full legal disclaimer.


